Lacebacks are a hallmark of conventional clinical practice, however controversy surrounds their use, and whether they are an advantage or a disadvantage. This blog explores the use of lacebacks, how they work, and the evidence surrounding them.
What are lacebacks?
A Laceback is a thin stainless steel auxillary wire commonly 0.009” (0.2 mm) diameter. They usually attach from the canine to the first molar, in a cross pattern between the teeth and under the archwire. There are two main methods of using lacebacks, passive and active:
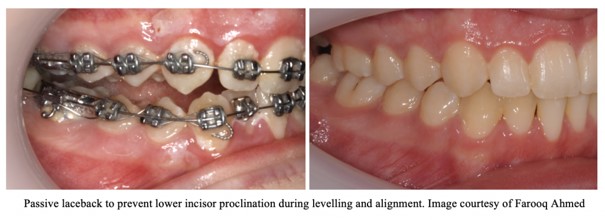
Passive laceback
The arch length between the canine and first molar are fixed. Without a laceback the expression of the straight wire force system (through the prescription and level and aligning) results in increasing the arch length between canine and molar, which prolines the incisors. This is most notable during the initial stages of levelling and aligning. In extraction cases, this results in round tripping with potential detriment to the gingival health and greater root resorption. Through a passive laceback the arch length is fixed, therefore the arch length cannot increase, the force system results in distal root tipping of the canine, which is usually desirable.
Uses of a passive laceback
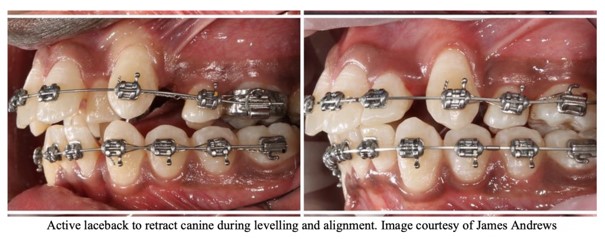
Active laceback
The laceback is tightened to produce an active force between the canine and first molar. This produces a high initial force (interrupted force) which reduces over the appointment interval. The canine is retracted during this process and the molars mesialise due to the reciprocal forces.
Uses of an active laceback
How do lacebacks work?
There are three main mechanics of how a laceback works:
1. Arch length fixation. The arch-length between the molar and canine is fixed, preventing the canine crown mesialising
2. Trampoline effect. A passive laceback can retract a canine through the effect of occlusal forces. Biting forces result in micro vertical movement of the dentition (trampoline), which result in the laceback bending momentarily. The bending of the laceback reduced the AP length of the laceback and retracts the canine. This process repeats many times with chewing / function
3. Canine center of rotation change. The biomechanical expression of point 1, the center of rotation of the canine moves to the canine bracket, with the moment expressing itself at mainly at the apical region.
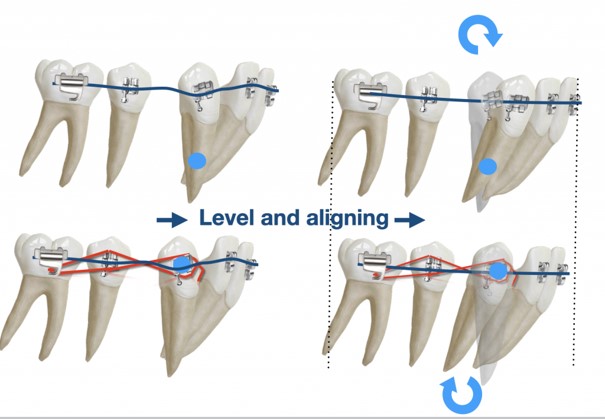
Should I use a laceback for a distally angulated canine?
Lacebacks are particularly useful in cases of disto-angular canines, and where incisor proclination is not desirable. Initial alignment with straight wire appliances result in significant proclination of the incisors. A laceback ensures the mesial tip of the canine bracket is not expressed by the canine crown tipping mesially, but instead the canine root moves distally, preventing the lower incisors proclining
It should be emphasized the preferential movement of distal root tip will result in greater anchorage loss through mesial molar movement (Irvine, 2004). For low anchorage cases this can be an excellent way to efficiently treat a case, conversely if anchorage requirements are high, other methods of anchorage preservation should be employed if using lacebacks
What does the evidence say?
The evidence about the effectiveness and efficiency of the use of lacebacks is controversial.In a classic study conducted by (Robinson, 1984) lacebacks were found to be effective in controlling lower incisors position with little additional loss of anchorage of the posterior segment.
A systematic review by Padhraig Fleming (Fleming et. al., 2013) has explored the topic further, the meta-analysis of two RCTs showed reduced lower incisor proclination by 0.5mm with the use of lacebacks in the lower arch, however the results were not statistically significant. There was greater anchorage loss with of 0.45 mm mesial movement of the molars, statistically non-significant.
Here is a table showing the results of the key studies about the topic, with the summary of the systematic review and meta- analysis by Fleming 2013
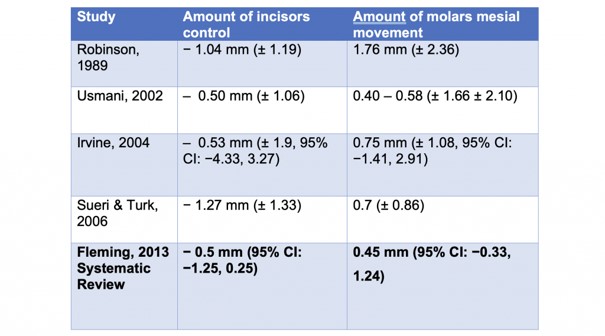
Systematic reivew of the effectiveness of lacebacks: Fleming 2013
Conclusion: Evidence is Meh, so why use them?
The use of lacebacks has been explored scientifically for incisor retraction and molar mesialisation, and have come up trumps. However the use of them in clinical practice prevails, including in our clinical practice. Although a systematic review has explored some aspects of laceback use, notably the evidence on active lacebacks, and disto-angular canines is absent. It also has to be taken into account a systematic review of two papers not ideal, a Cochrane systematic review was considered into lacebacks in 2016 however it was discontinued due to a lack of studies (Kozel et al., 2016). With this in mind the decision to use lacebacks still remains one driven by empirical evidence.
References
McLaughlin RP, Bennett JC. The transition from standard edgewise to preadjusted appliance systems. J Clin Orthod 1989; 23: 142–153.
Irvine R, Power S, McDonald F. The effectiveness of laceback ligatures: a randomized controlled clinical trial. J Orthod 2004; 31: 303–311.
Usmani T, O’Brien KD, Worthington HV, Derwent S, Fox D, Harrison S,
et al. A randomized clinical trial to compare the effectiveness of canine lacebacks with reference to canine tip. J Orthod 2002; 29: 281–286; discussion 77.
Fleming PS, Johal A, Pandis N. The effectiveness of laceback ligatures during initial orthodontic alignment: a systematic review and meta- analysis. Eur J Orthod 2012: cjs033.
Halimi A, Benyahia H, Doukkali A, Azeroual MF, Zaoui F. A systematic review of force decay in orthodontic elastomeric power chains. Int Orthod 2012; 10: 223–240.
Elhussein MA, Sandler PJ. Effective Derotation of canines and premolars. J Clin Orthod 2016; 50: 700.
KOZEL, J. A., MACEDO, C. R. & ATALLAH, Á. N. 2016. Laceback ligatures for controllinganchorage in patients undergoing fixed orthodontic treatment. The Cochrane Database of Systematic Reviews, 2016.
Contributions
We hope you have enjoyed this blog, This blog started with a conversation between Kerolos AlHakeem, Farooq Ahmed and James Andrews, to follow more conversations, clinical tips and commentaries on orthodontics please check us out on Instagram:
Kerolos AlHakeem’s Instagram page @dr_al_hakeem
James Andrews’ Instagram page @dr.jamesandrews